




Recently we hosted a course on small intestinal bacterial overgrowth (SIBO) with Dr Jason Hawrelak called Demystifying SIBO. True to its name, Dr Hawrelak spoke frankly about the flaws in SIBO testing and demystified many of our long-held beliefs about SIBO in clinical practice.
We feel very lucky to have these conversations with leaders in their fields, to constantly push us to learn, adapt and evolve our clinical thinking.
One of the things that Jason really got us thinking about was the pros and cons of different types of substrates used in SIBO breath testing. Breath testing is notoriously tricky, but the trouble is, it is the only tool we have to hand, apart from a clinical biopsy, to investigate the ‘where’ of the bacteria in our gastrointestinal tract.
Different bacteria metabolise different substrates, so testing with just one substrate can miss some bacterial colonies, and other substrates such as lactulose can speed up transit time, making the cut-off point from where we calculate the rise in gas, hard to read. Even with all these cons, the flip side of not testing at all can also mean the client misses out on a solution that could work for them.
Using all three substrates when testing for SIBO (lactulose, fructose and glucose) on consecutive days may allow for a clearer picture of what is going on. Even then, the information is limited, as it is only really telling us what is going on in the small intestine. One thing we know about the intestines, is that they are not isolated from each other – if there is something ‘wrong’ in one area, it will have major impacts on the other areas of the intestine. In other words, SIBO is part of a whole digestive ecosystem disorder.
With all considering, we have concluded as a team that SIBO is an ecosystem disorder, and thus our suggested approach to testing is to use either a fructose or glucose-based breath test for the SIBO (due to less false positives), combined with an overall stool ecology test, such as the GI EcologiXTM. Doing this provides information about the entire intestine and it can give you more targeted information on how the SIBO has developed and sustained itself.
Notes on breath testing – when possible SIBO might be LIBO (lower intestinal bacterial overgrowth)
One thing to watch in test results for SIBO (with any substrate) is a high baseline reading that drops to normal levels again until around the 90-minute mark (transition to large bowel occurs around this point in most substrates). After ruling out incorrect preparation diet, the next thing to consider is large intestinal bacterial overgrowth (LIBO), or what we commonly refer to as dysbiosis.
The multiple causative agents of SIBO
SIBO can be triggered by multiple factors. The most common factors are events such as food poisoning, and one, or more of the many reasons for poor motility of the small intestine.
Key question: When assessing SIBO, the main thing we should be asking ourselves is how did the bacteria get there and what is the perfect storm of conditions that is permitting them to stay long term?
SIBO is well known for its high re-occurrence rate, so it is of utmost importance to try and dig deeper into what the compounding and provoking factors might be to ensure long-term success.
Some of the many things to think about, assess and address are:
- Structural issues – adhesions from operations or endometriosis, connective tissue diseases such as Ehlers-Danlos Syndrome, hypermobility or rheumatoid arthritis, scar tissue from previous operations or skeletal mechanical issues impacting muscular tone, bowel shape or enervation to the GIT
- Nervous system issues and damage to the migrating motor complex (MMC) of the small intestine – functional constipation, damage to the MMC after food poisoning, stress causing poor vagal tone and blood supply to the intestine, diseases that damage the nervous system such as Parkinson’s disease or multiple sclerosis.
- Poor digestive function – such as low HCL acid – either from stress or antacid use, Helicobacter pylori infections, low digestive enzyme function (can be related to stress, or diseases such as coeliac disease), poor bile flow due to gall stones or other disorders.
Using stool testing with SIBO
Stool testing allows for an assessment of the many different factors that can contribute to the causation and duration of SIBO. Things like digestive function, imbalance of specific bacterial communities, and the presence or absence of host-microbial patterns can all help us to get a broad picture of the case and enable us to use targeted therapies and interventions to help manage and prevent re-occurrence.
Bacterial and host patterns in the GI EcologiXTM with people with SIBO
When I interpret a GI EcologiXTM with a SIBO case, there are few key patterns I am looking for:
- How is the digestive function?
I would be looking at the Pancreatic Elastase to see if it is low. It can be a bit of a chicken/egg scenario in SIBO – as sometimes SIBO can lead to low pancreatic elastase, or low pancreatic elastase and the resulting poor digestive breakdown can lead to SIBO. Either way, poor digestive function can be a major reason the bacteria overgrow in the first place and would need addressing. - Methanogenic bacteria
One of the high methane gas producers in the bowel is Methanobrevibacter smithii. In SIBO, it will more likely present with constipation, but it can also present with diarrhoea, bloating, pain and flatulence. On a breath test, if baseline methane is raised, but it doesn’t raise again for the rest of the test until after 90 minutes, it shows you the methanogenic bacterial overgrowth is more likely in the large intestine. A small number of methanogens may be normal in some individuals, but moderate to high levels are normally indicative of excessive gas production, which can be associated with constipation, diarrhoea, abdominal pain, IBS and IBD. Methanogens grow less in a low pH environment and they are limited by their inability to degrade sugars. This means they are obligate cross-feeders, meaning they are dependent on the products of other carbohydrate degraders for their survival. - Sulfidogenic bacteria
One of the downfalls of SIBO breath testing is that it cannot evaluate the amount of hydrogen sulphide in the intestine. Hydrogen sulphide can cause symptoms of diarrhoea, bloating, pain, gas and inflammation. The most common bacteria associated with hydrogen sulphide gas production are Desulfovibrio and Bilophila wadsworthia, and to a small extent Fusobacterium. These bacteria enjoy a high fat/high bile environment and are normally find in diets that are rich in saturated fats, especially those found in dairy, meat and coconut oil1. In an omnivore diet, we would expect Bilophila wadsworthia to sit normally between very low to low, almost as a commensal. Any higher than this, or if it is combined with Desulfovibrio, it may be associated with the aforementioned symptoms of hydrogen sulphide. These bacteria source their sulphur from the amino acids cysteine, methionine and taurine from animal products and to a small extent inorganic sulphur in cruciferous vegetables. Sulphate may also be generated from the breakdown of endogenous sulphur containing mucins, which can only be utilised when mucin degrading bacteria such as Bacteroides vulgatus liberate them from the mucin lining2.
More interpretive resources (logged-in):
WEBINAR: How to navigate a GI EcologiX report
RESOURCE: How to interpret a GI EcologiX report
Other bacteria involved in SIBO
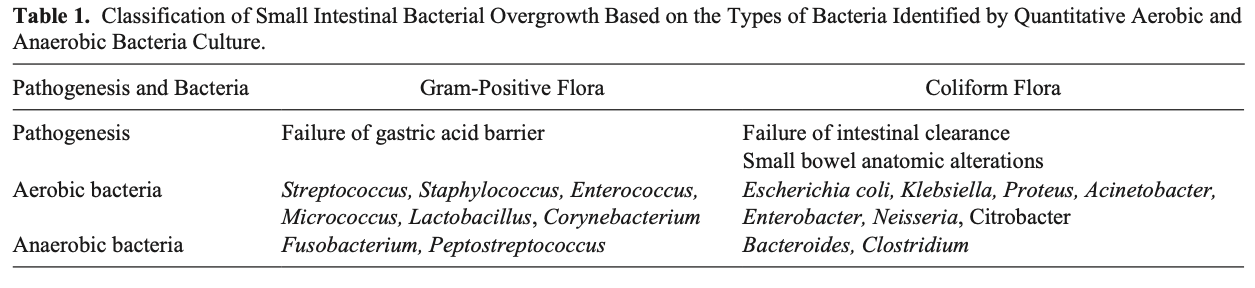
The small intestine and stomach has its own microbiota, but with low abundance. Overgrowth of local bacteria (or oral bacteria) can occur with sub-optimal stomach acid function, which is a common effect of taking antacid medications. Bacteria such as Streptococcus, Staphylococcus, Enterococcus, and Lactobacilli may all be indicated. Oral bacteria such as Fusobacterium nucleatum or Peptostreptococcus may also play a role in the overgrowth. Bacteria may also overgrow due to a lack of clearance of the small intestine, or changes in structure. In this case, you might see high numbers of E. coli, Klebsiella, Proteus, Bacteroides or Clostridium3.
Other factors
The great thing about using a combined approach when looking for SIBO is you might just find more than you realised in the GI EcologiXTM. Inflammation, degradation of the mucin lining, poor host defences, pathogens, issues with diversity, poor digestive function, complications with fungi, are all extra things that you can evaluate to help you to formulate your whole ecosystem gut support plan and support someone back to their journey of wellness.